.svg)
.svg)

.svg)

ترجمه مقاله بهبود تعامل، کار گروهی و عمل در زمان وقوع حالت اضطراری ناتوانی در لوله گذاری - نشریه اشپرینگر

عنوان فارسی
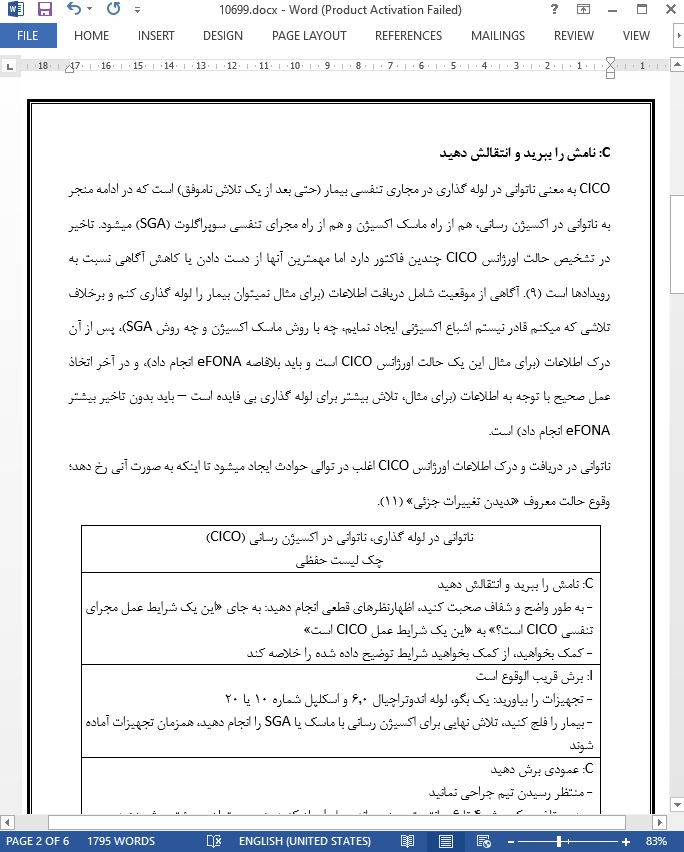
بهبود تعامل، کار گروهی و عمل در زمان وقوع حالت اضطراری ناتوانی در لوله گذاری، ناتوانی در اکسیژن رسانی (CICO) با بکار گیری CICO به عنوان روش کمک شناختی حفظی
عنوان انگلیسی
Improving communication, teamwork, and action during a ‘‘cannot intubate cannot oxygenate (CICO)’’ emergency: employing CICO as a cognitive aid mnemonic
صفحات مقاله فارسی
6
صفحات مقاله انگلیسی
6
سال انتشار
2018
رفرنس
دارای رفرنس در داخل متن و انتهای مقاله
نشریه
اشپرینگر - Springer
فرمت مقاله انگلیسی
pdf و ورد تایپ شده با قابلیت ویرایش
فرمت ترجمه مقاله
pdf و ورد تایپ شده با قابلیت ویرایش
فونت ترجمه مقاله
بی نازنین
سایز ترجمه مقاله
14
نوع مقاله
ISI
نوع نگارش
EDITORIALS
نوع ارائه مقاله
ژورنال
پایگاه
اسکوپوس
ایمپکت فاکتور(IF) مجله
3.278 در سال 2019
شاخص H_index مجله
90 در سال 2020
شاخص SJR مجله
0.894 در سال 2019
شناسه ISSN مجله
0832-610X
شاخص Q یا Quartile (چارک)
Q1 در سال 2019
کد محصول
10699
وضعیت ترجمه منابع داخل متن
درج نشده است ☓
ضمیمه
ندارد ☓
بیس
نیست ☓
مدل مفهومی
ندارد ☓
پرسشنامه
ندارد ☓
متغیر
ندارد ☓
رفرنس در ترجمه
در داخل متن و انتهای مقاله درج شده است
رشته های مرتبط با این مقاله
پزشکی
گرایش های مرتبط با این مقاله
پزشکی ریه یا پولمونولوژی، بیهوشی
مجله
مجله بیهوشی کانادایی - Canadian Journal of Anesthesia
دانشگاه
گروه بیهوشی، فارماکولوژی و درمان، دانشگاه بریتیش کلمبیا، ونکوور، کانادا
doi یا شناسه دیجیتال
https://doi.org/10.1007/s12630-018-1193-0
۰.۰
(هنوز امتیازی ثبت نشده است)